Bleeding could occur from the cervix and may require a
blood transfusion, a return to the operating room or other
measures, such as vaginal packing, to control the bleeding.
Damage and narrowing of the cervix could occur which
can cause painful periods and difficulty in labour.
Complete closure of the cervical canal, which can cause
difficulty in having a period, pelvic pain, infertility and
difficulty obtaining a pap smear. The cervical canal might
require dilatation under anaesthetic and on some occasions
it may require having a hysterectomy (removal of uterus).
The cervix may be weakened which can lead to early
pregnancy loss and the occasional need to strengthen
the cervix during a pregnancy by the insertion of a special
stitch (cervical cerclage). The risk of preterm labour is also
increased. Women who have had a prior LLETZ procedure
may have to have their cervix length measured regularly by
ultrasound during pregnancy to ensure it is not shortening
or opening too early.
Blood clot in the leg causing pain and swelling. In rare
cases, part of the clot may break off and go to the lungs.
Small areas of the lung can collapse, increasing the
risk of chest infection. This may need antibiotics and
physiotherapy.
Heart attack or stroke could occur due to the strain on
the heart.
Damage to surrounding organs such as bladder, rectum
etc. and further surgery may be required to rectify this.
Subsequent infertility.
Miscarriage or premature labour can occur, usually from
12 weeks onward in future pregnancies, as a result of
weakness of the cervix. This is relatively more common if
this procedure has to be done more than once .
Hysterectomy (removal of uterus) if bleeding is unable to
be controlled.
(Source: https://www.health.qld.gov.au/__data/assets/pdf_file/0035/147887/obst_gyna_23.pdf)
Wow, that's a long list! So those are the official complications, as found in the consent form in the source link above.
So is that all we have to worry about? Looking at women's stories in the media and online, it seems not, sadly.
Women have complained of suffering from weakened stomach muscles, a loss of libido (desire for sex), loss of orgasm and painful sex.
(Source: https://www.dailymail.co.uk/health/article-5960067/The-women-say-treatment-smear-test-RUINED-sex-lives.html)
So, a treatment which isn't even for cancer, but rather some cell changes that just might become cancer, could leave you infertile, in constant pain, lacking a sex drive, or orgasmic ability.
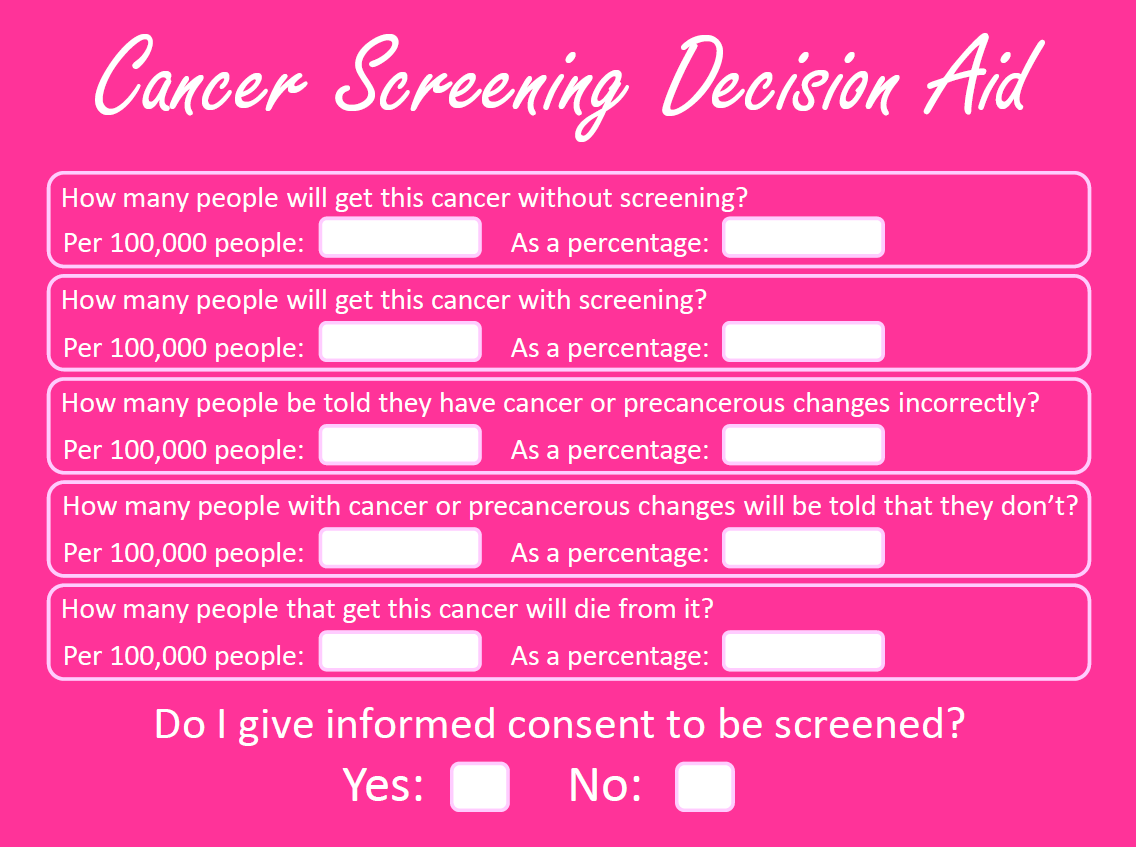
Should you accept this treatment?
That's really up to you. There is a risk of cancer, but there's also a chance that you'll be absolutely fine.
But if you do, do so knowing all the risks and benefits. This information is not always given to women, and it should be.