Sounds familiar, right? It’s the title of the little green
information leaflet that is sent out with your invitation to attend cervical
screening. Let’s look at that. It’s an invitation, and you can decide whether
to take part or not. It’s a choice.
How do you make that choice? Well the leaflet has some
information in it, but not all the information we need to make an informed
decision, as you’ll know from previous posts on this blog. Let’s take a look at
the numbers.
Organised cervical screening was introduced in the UK in 1988.
Mortality rates for cervical cancer were already in decline before that. Let’s
see how the screening test reduced cervical cancer deaths (source: Cancer
Research UK):
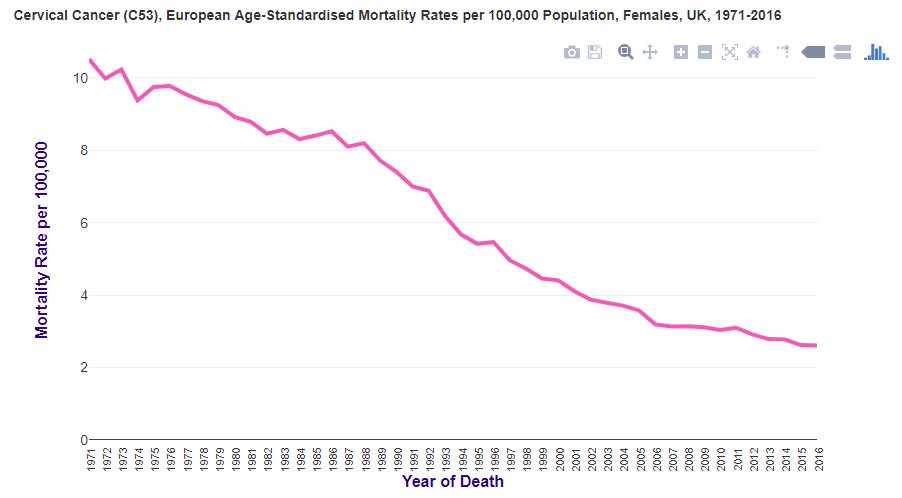
Well, I suppose it went down a little bit faster, but it was
already going down. Not a very dramatic change is it?
Why is that?
Cervical screening isn’t, as the leaflet agrees, a test for
cancer. It is a test for abnormal cells that might, just might, become cancer.
If you have abnormal cells detected with screening, you’ll likely worry, but
let’s look at how likely those cells are to become cancer (invasion):
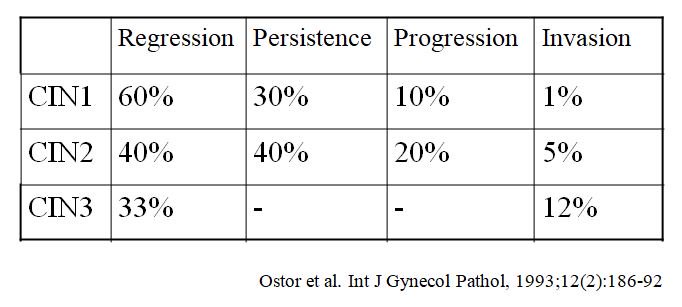
Ok, so now we can breathe a sigh of relief, well, depending
on how abnormal our cells were. This is expressed as the CIN level, ranging
from 1 to 3. CIN stands for cervical intraepithelial neoplasia. It’s not
cancer, but sometimes these cells can change into cancer. In the table above,
you can see how likely this is to happen, in the “invasion” column – this is the
risk of the cells becoming cancer.
So these abnormal cells that they’re looking for don’t
always become cancer. In fact, looking at the table above, it’s actually quite unusual
for this to happen.
What causes these abnormal cells, which might go on to cause
cervical cancer? The answer is HPV (source: https://embryo.asu.edu/pages/harald-zur-hausens-experiments-human-papillomavirus-causing-cervical-cancer-1976-1987).
HPV, or human papillomavirus, is a common virus, with many subtypes. Some cause genital warts, whereas others can
cause abnormal cells, which may become cancerous. HPV subtypes 16 and 18 are
the primary causes of cervical cancer. These HPV subtypes can be prevented with
vaccination. HPV is sexually transmitted, from penetrative sex, and also oral
sex. It is also implicated in cancers of the mouth, throat, penis and anus.
Anyway, how accurate is cervical screening?
In a previous post on this blog, we looked at sensitivity,
and specificity. Let’s see what that looks like for cervical screening:
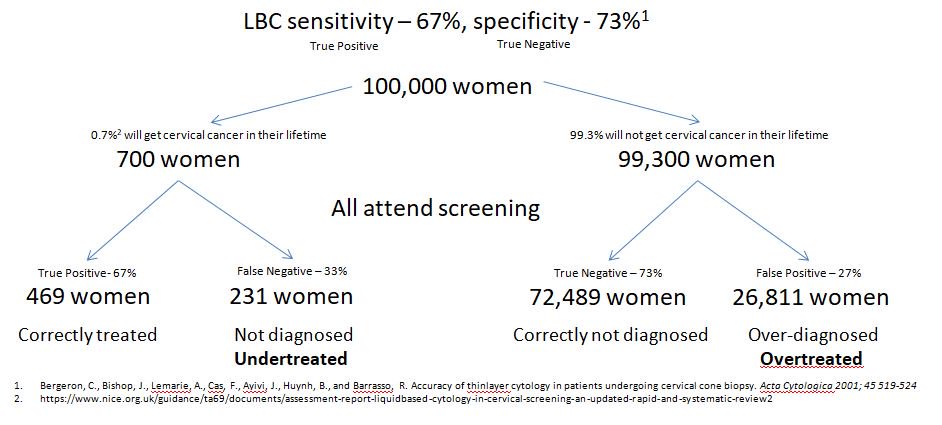
LBC stands for liquid based cytology, and is the most up-to-date
method to collect smears. As we can see from this diagram, screening would
wrongly tell 231 women with cancer, that they don’t have it. It would also tell
26,811 women with no disease, that they have cancer.
This is a simplified diagram, as it only takes women with
actual cancer into account, not all those abnormal cells (CIN1, 2 & 3)
mentioned earlier. If we factored those in, given that up to 7.7% of women
might have abnormal cells at any one time (source: https://www.ncbi.nlm.nih.gov/pubmed/24305750),
that’s another 7,700 women that could be given false negative, or false
positive result. Even though those cells only have a small chance of becoming
cancer. This could result in treatment that women don’t need.
So what does this look like?
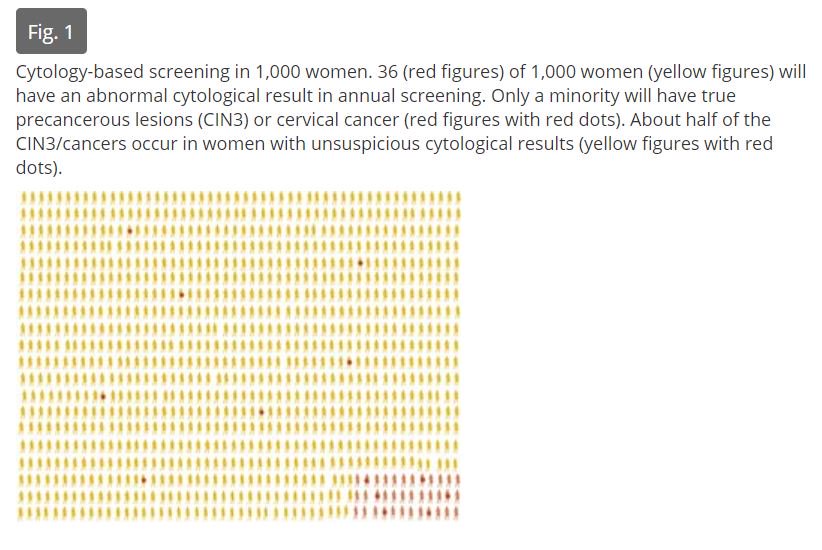
It’s a little hard to see, but when a smear test is read,
and the result sent back, of the 36 women with high-grade abnormal cells, or
cancer, detected, only 6 of those 36 will actually
have high-grade abnormal cells, or cancer. The rest do not. Of the remaining 964 women told that
they are fine, 7 of them will actually
have high-grade abnormal cells, or cancer, and be told that they don’t. It’s a
bit like flipping a coin for a correct diagnosis.
What about those women without abnormal cells, who are told
that they have abnormal cells, or cancer, erroneously?
Let’s take a look at that:
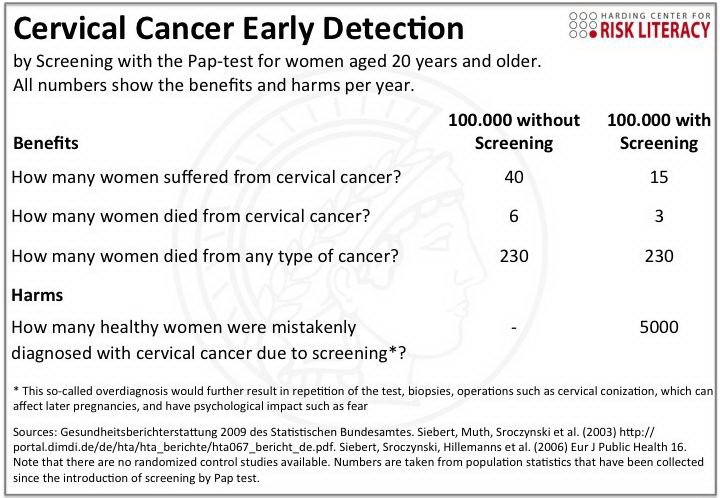
Without screening 6 per 100,000 women will die from cervical
cancer (0.006%), with screening 3 per 100,000 women will die from cervical cancer
(0.003%). This is a 50% relative
risk reduction, but really the actual risk
reduction is 0.003% (0.006% - 0.0003%)
However, with screening, 15 women would still develop cervical cancer, and 5000 women (5%) would be diagnosed with cancer
incorrectly, and treated.
So, what’s the problem with treating those 5000 women
incorrectly? What’s the harm?
CIN, and cervical cancer have different treatments. Cervical
cancer treatment might result in a hysterectomy, the removal of the uterus,
leaving women infertile, but could well save their lives. Cervical cancer
should be treated, as it can spread.
CIN treatment aims to remove the abnormal cells before they
become cancer (remember the risk of this happening from above). Such treatments
are LLETZ (Large loop excision of the transformation zone), Cone biopsy, Laser
therapy, Cold coagulation (it’s not cold, it’s actually very hot!), and Cryotherapy
(this one is actually cold). The aim of these treatments is to remove the
abnormal cells from the cervix.
Whilst not everyone suffers from side effects from these
treatments, there is always a risk of death from a general anaesthesia (if
required) which is 1 per 100,000 patients (source: https://www.nhs.uk/conditions/general-anaesthesia/),
along with pain, bleeding and discharge.
Some treatments can cause cervical stenosis, where the
cervix becomes tightly closed, prevent sperm from reaching the uterus, and
fallopian tubes, causing infertility. Conversely, some treatments can cause weakening
of the cervix, which is a muscle, increasing the risk of preterm birth. (Source:
https://www.macmillan.org.uk/information-and-support/diagnosing/how-cancers-are-diagnosed/cervical-screening/treating-cin.html#3817)
So, should you get screened for cervical cancer?
The answer
is, it’s your choice. Being armed with all the relevant facts should allow you
to make your own decision, based on your own personal situation, as to whether you
wish to participate, or not.
Don’t be bullied into it by friends or doctors, make your
own, informed, choice.




It's amazing how often I share this info with women and they reply "nothing will put me off testing. It's so important."
ReplyDeleteIt's very clear that many don't actually understand data and statistics at all. They cannot refute the evidence but parrot a response they've been brainwashed to give.